Cryptococcus neoformans is a ubiquitous environmental encapsulated fungus.
The fungus abundantly inhabits the soil and is found in bird droppings.
In nature, neoformansvar. gattii (serotypes B and C) has been isolated from decaying wood in the red gum group of eucalyptus trees.
neoformans var. neoformans (serotypes A and D) has been isolated most frequently from soil contaminated with pigeon or other bird droppings.
It has also been recovered from old dried accumulations of bird droppings in buildings, but has not been found in fresh wet droppings.
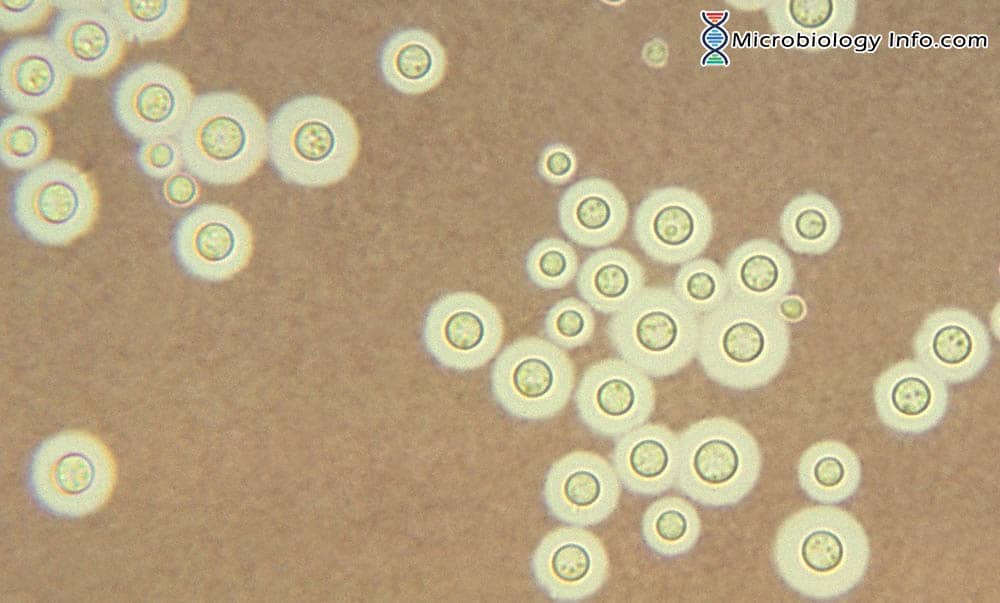
Morphology
neoformans is an encapsulated, environmental yeast.
Cryptococcus neoformans is a round or oval yeast measuring 4–6 µm in diameter, surrounded by a capsule that can be up to 30 µm thick.
Spherical fungus which reproduces by budding at any point on the surface, sometimes producing several buds simultaneously at various points.
Buds attached to the parent cell by a thin wall and a very narrow pore.
Under conditions of rapid growth, the buds break free of the parent cell earlier and the cells found in tissue and in culture vary widely from 4-20 µm in diameter.
Thin cell wall, collapses on drying or sudden change in osmotic pressure.
Cell surrounded by mucoid polysachharide capsule which are either thin or equal in thickness twice the cell radius.
Capsule thickness varies with fungus strain and is greater in tissue than in culture.
Capsule production increased by the growth in 1% peptone solution.
Life cycle involves 2 different forms: asexual and sexual
Asexual forms (haploid and unicellular) exists as yeast cells and reproduces by budding.
Sexual cycle represented by
Conjugation of two yeast cells
Production of long hyphae with clamp connections
Formation of basidium
Basidia produce sessile basidiospores by repetitious budding that results in chain of basidiospores.
Dalmau Plate Culture: Budding yeast cells only. No pseudohyphae present.
Bird Seed Agar:Colonies appear as dark brown in color as colonies selectively absorb a brown pigment from the media.
Canavanine Glycine Bromothymol Blue (CGB) Agar: No growth or color change.
Creatinine Dextrose Bromothymol Blue Thymine (CDBT) Agar: used to differentiate neoformans var. neoformans and C. neoformans var. grubii.C. neoformans var. neoformans grows as bright red colonies, turning the medium a bright orange after 5 days while no color change is observed for C. neoformans var. grubii.
Epidemiology
On the basis of differences in a number of mycological, biochemical, ecological and epidemiological characteristics, isolates of neoformans can be divided into two varieties, C. neoformans var. neoformans and C. neoformans var. gattii,
Isolates of neoformans can also be divided into five serotypes, termed A, B, C, D and AD (both A and D determinants present) on the basis of antigenic differences between their capsular polysaccharides.
The two varieties, var. neoformans and var. gattii, are comprised of serotypes A, D and AD, and serotypes B and C, respectively.
The two serotypes differ in their geographical distribution: human infections with serotype A have a global distribution while infections with serotype D are more prevalent in certain geographical areas such as northern Europe.
neoformans var. neoformans has a more restricted distribution with infections being more prevalent in Europe, including France, Italy and Denmark, where it accounts for 30% of isolates.
neoformans is found worldwide, is associated with avian excreta (particularly that of pigeons), and causes the vast majority of human infections.
Moreover, neoformans var. neoformans infections are more strongly correlated with older patients, the skin, and the use of corticosteroids.
Cryptococcus neoformansneoformans is the major cause of cryptococcal disease worldwide. Serotype A is the most common serotype infecting AIDS patients.
neoformans var. grubi i has a worldwide distribution, causing 95% of all C. neoformans infections.
It has been isolated from various sources in nature and is noted for its association with accumulations of avian guano, especially with pigeon excreta.
The fungus has also been isolated from the dung of caged birds including canaries, parrots and budgerigars.
Other environmental isolations of neoformans var.grubii include rotting vegetables, fruits and fruit juices, wood, dairy products and soil.
The spectrum of cryptococcal disease ranges from self-limiting cutaneous infections to fatal systemic ones.
Systemic disease is contracted by inhalation of the infectious particle which leads to a primary pulmonary infection.
It can remain latent for extended periods of time, but emerges and disseminates when the host becomes immunocompromised.
Upon dissemination the organism shows particular tropism for the central nervous system (CNS), frequently causing fatal meningitis termed as Cryptococcal meningitis.
Virulence factors
1. Capsule
The outer polysaccharide capsule composed primarily of a high molecular weight polysaccharide that has a backbone of -1,3-D-mannopyranose units with single residues of ß-D-xylopyranosyl and ß-D-glucuronopyranosyl attached of neoformans is the most potent virulence factor which also allows it to evade the immune system.
The capsule is composed primarily of two large polysaccharides, glucuronoxylomannan (GXM) and glucuronoxylomannogalactan (GXMGal).
2. Melanin production
The organism’s ability to form a brown to black pigment on a medium (such as birdseed or caffeic acid agar) that contains diphenolic compounds is one of the characteristic that differentiates pathogenic isolates of neoformans from nonpathogenic isolates and other Cryptococcus species.
In the presence of appropriate precursors neoformans produces melanin which provides protection from environmental stresses including antifungal compounds.
Melanin confers protection against phagocytosis and oxidative killing by macrophages and contributes to extrapulmonary dissemination.
3. Extracellular enzymes
Laccases and phospholipase B are located in cell wall and mediate melanin formation and cell wall integrity respectively.
Phospholipase also contributes to fungal invasion of host lung tissue and dissemination.
Phospholipases cleave phospholipids to produce various biologically active compounds.
These enzymes alter the microenvironment of infection, hence favoring neoformans survival in the host.
4. Cell wall changes and adaptation to the host
In addition to the production of specific enzymes and structures that favor pathogen survival, neoformans also actively modulates its cell wall in response to specific signals directed towards host.
This remodeling of the cell wall results in immune evasion by shielding more immunogenic surface features.
Additionally, the cell wall serves as the point of capsule attachment or capsule binding.
neoformans is unique among human fungal pathogens as the cell wall comprises of carbohydrates, including chitin, chitosan, and glucans.
Since, the neoformans cell wall is comparatively rich in chitin and chitosan in comparison to other pathogenic fungi, chitin exposure likely plays a significant role in cryptococcal pathogenesis and immune recognition.
5. Extracellular vesicles
Various factors which are found associated with neoformans pathogenesis must be transported from intracellular sites where synthesis occurs to locations on the cell surface or outside of the plasma membrane.
Several elements of unconventional secretion mechanisms are found involved in the export of capsule and other virulence associated molecules.
Such structures have been visualized as microvesicles, present inside the cell as well as in the extracellular space.
Numerous investigators in their study have described the role of these microvesicles in neoformans pathogenesis, especially in the transport of substances associated with classical virulence factor expression.
Microvesicles contain many substances: capsule precursors, melanin, and secreted enzymes.
Microvesicles, also termed as “virulence bags” are quite stable, and they appear to be able to act locally on either the extracellular surface of the microorganism or to influence the interaction with host cells.
Cryptococcus-derived microvesicles in their pathogenesis process favor alterations of the blood brain barrier which then allow neoformans to cross the barrier and make an entry to the central nervous system.
Pathogenesis
The usual mode of Cryptococcal infection in humans is inhalation of aerosolized neoformans cells as a result of environmental exposure.
The incubation period is unknown and could be weeks, months or even longer.
In healthy individuals Cryptococcus neoformans infection is usually cleared, or can remain in a latent state for prolonged periods of time.
The activation of innate and adaptive cellular immune responses in healthy individuals limits the severity of the infection to an asymptomatic and often self-resolving pulmonary infection.
On contrary in the immunocompromised individuals, hematogenous dissemination of neoformans from the lungs to the central nervous system can lead to cryptococcal meningoencephalitis which is a life-threatening complication requiring aggressive chemotherapeutic intervention.
neoformans proliferates within host phagocytic cells which may confer advantages in terms of dissemination and immune protection.
Initial interactions of the yeast with host cells are mediated by an adhesin and also involve host recognition of fungal capsule components.
Once adherent cells are internalized, they traffic to the vacuole where they are able to survive and replicate and the host immune status greatly influenced the outcome of internalization.
The best ultimate outcome is fungal death; alternatively either cryptococci may continue to replicate within the host cell, or they may exit either by a lytic process lethal to the host cell or by a non-lytic process that leaves both cells intact.
Entry to the CNS is a key step in pathogenesis of Cryptococcus neoformans.
Various reports and studies suggest that both internalized and free Cryptococci are able to cross the blood-brain barrier to reach the brain, either by transcytosis through barrier epithelial cells or between them via breach of the tight junctions or a combination of both events may also occur.
Clinical manifestations of Cryptococcus neoformans
1. Pulmonary Cryptococcosis
Up to 30% of immunocompetent individuals develop no symptoms following inhalation of neoformans and their infection remains unrecognized until it has spread to other organs.
Additionally, patients with chronic lung disease, such as bronchitis and bronchiectasis, may also have asymptomatic colonization, withCryptococcus being isolated from their sputum over many years.
The environmental exposure to neoformans result in a subclinical cryptococcosis and normal individuals may experience a self-limiting pneumonia with accompanying sensitization.
Most primary infections exhibit no diagnostic symptoms and are usually explained only by routine chest x-ray.
Clinical presentations also depend on the characteristics of the immunological competency of the patients.
Unlike normal individuals, most immunocompromised patients exhibit symptoms including fever malaise, chest pain, weight loss, dyspnoea, night sweats and cough. .
The most frequent radiological findings are well-defined, non-calcified, single or multiple nodular lesions.
On the other hand, less common findings include indistinct to mass-like infiltrates, hilar and mediastinal lymph node enlargement, pleural effusions and cavitation.
In the cases where primary infections are not resolved, it often leads to invasive pulmonary cryptococcosis, further leading to a more chronic pneumonia progressing slowly over several years.
Chronic pulmonary cryptococcosis also increases the risk of dissemination to the central nervous system.
2. CNS infections (Cryptococcal meningitis)
Cryptococcus neoformans continues to be an important cause of morbidity and mortality, and is considered as the most common central nervous system (CNS) mycosis in immunocompromised patients, in particular those with AIDS.
Dissemination of infection from pulmonary region to the brain and meninges is the most common clinical manifestation shown by Cryptococcus neoformans and includes meningitis, meningoencephalitis or expanding cryptococcoma.
Meningitis is the most common clinical form which accounts upto 85% of the total number of cases.
Symptoms usually develop slowly over several months, and initially include headache, followed by drowsiness, dizziness, irritability, sensitivity to light, confusion or changes in behavior, nausea, vomiting, neck stiffness and focal neurological defects, such as ataxia.
Headache is the most common presenting symptom and the pain is dull, bilateral and diffuse.
Fever is often minimal or nearly absent until late in the course of the infection.
In later stages of infection, diminishing visual acuity and coma may also occur.
Meningoencephalitis due to invasion of the cerebral cortex, brain stem and cerebellum is an uncommon, rapid fulminate infection, often leading to coma and death within a short time.
Cryptococcoma is a rare entity, often characterized by localized, solid, tumor-like masses, usually found in the cerebral hemispheres or cerebellum, or more rarely in the spinal cord.
Symptoms are consistent with an expanding intracranial mass and include headache, drowsiness, nausea, vomiting, mental changes, slurred speech, double vision, unsteadiness of gait, coma, paralysis and hemiparesis.
3. Cutaneous Cryptococcosis
Hematogenous spread of neoformans gives rise to skin lesions in 10-15% of patients with disseminated cryptococcosis infections.
Cutaneous lesions are common clinical manifestations in HIV-infected individuals with cryptococcosis and considered as the second most common site of disseminated cryptococcosis.
Primary cutaneous cryptococcosis in the form of ulcerated lesions or cellulitis occasionally occurs, especially in immunosuppressed patients.
Secondary cutaneous infections occur in patients with disseminated cryptococcosis and often indicate a poor prognosis.
In some cases these lesions are the earliest clinical sign of infection and are often located on the face and scalp, but may occur on the trunk or limbs.
Lesions usually begin as small papules (single or multiple nodules) that subsequently ulcerate, but may also present as abscesses, erythematous nodules, or cellulitis.
Lesions often occur on the head and neck and may present as papules, nodules, plaques, ulcers, abscesses, cutaneous ulcerated plaques.
Anal ulceration may also occur.
4. Ocular Cryptococcosis
The ocular signs of cryptococcosis are generally uncommon and is usually a outcome of dissemination.
The most common manifestations of ocular cryptococcosis include papilledema (optic disc swelling) and optic atrophy, due to raised intracranial pressure.
5. Cryptococcosis of Bone (Osteomyelitis)
Osteomyelitis occurs in 5-10% of patients with disseminated cryptococcosis and may involve bony prominences, cranial bones and vertebrae.
Most patients present with a single isolated lesion, spine being the commonest site of involvement with patient complaining of local pain and soft tissue tenderness at the affected site.
The lesions are lytic and symptoms of dull pain on movement are reported.
Radiographs reveal well-defined osteolytic lesions without marginal sclerosis or periosteal change and CT scans can be used to define the extent of bone involvement.
Occasional cases of arthritis have also been reported which mostly involves the knee joint.
6. Other forms of Cryptococcosis
In patient with disseminated infections, Cryptococcus neoformans is often isolated from urine.
Occasionally, signs of pyelonephritis or prostatitis may be observed in patients.
Additionally, other rare forms of cryptococcosis include adrenal cortical lesions, endocarditis, hepatitis, sinusitis, and localized oesophageal lesions.
Thin wet film under a coverslip using India ink for exudates and body fluids to demonstrate encapsulated yeast cells.
Sputum and pus are subjected to 10% KOH preparation prior to India ink staining.
For tissue sections, to demonstrate the polysaccharide capsule, PAS (Periodic acid-Schiff- stain), GMS (Grocott’s methenamine stain) and H&E, mucicarmine stain are often used.
Examine for globose to ovoid, budding yeast cells surrounded by wide gelatinous capsules.
Positive sputum specimens should be considered potentially significant, even though Cryptococcus may also occur in respiratory secretions as a saprophyte.
Basically, all patients with a positive microscopy for cryptococci, from any site should be investigated for disseminated disease, especially by culture and antigen detection.
3. Culture
The organism grows well on standard microbiological media.
It grows best at 30°C-35°C and in suspected case, prolong incubation of plates in suspected cases for up to 2 weeks is recommended.
Inoculate specimens onto primary isolation media, like Sabouraud’s dextrose agar.
Observe for translucent, smooth gelatinous colonies, later becoming very mucoid and cream in color.
4. Serology
The method of choice or the most reliable methods for diagnosing patients with cryptococcal meningitis is detection of cryptococcal capsular polysaccharide antigen in spinal fluid.
In AIDS patients with cryptococcosis, cryptococcal antigen can be detected in the serum in nearly 100% of cases. However, in non-AIDS patients antigen detection in serum is less sensitive with only about 60% of patients with cryptococcosis reported as being positive.
Tests such as latex particle agglutination (LPA) and enzyme-linked immunosorbent assay (ELISA) have been marketed for the detection of antigen in serum, CSF, urine and BAL fluid specimens.
These tests are specific; however, false-negative results can occur if the organism load is low or if the organisms are not well encapsulated.
A serum antigen titre of 1:8 or greater is considered strong presumptive evidence of neoformans infection. A negative serum antigen test result does not exclude the diagnosis of cryptococcosis, particularly if only a single specimen has been tested and the patient has symptoms consistent with the infection.
Levels of antigen in the CSF often decline with treatment, but the test can remain positive for several weeks.
Antibodies to neoformans can often be detected in patients with localized or past infection, but are seldom found in patients with untreated meningeal or disseminated infection.
Treatment
In patients with asymptomatic infections or mild-to-moderate pulmonary infections, the treatment is usually fluconazole.
In patients with severe lung infections or infections in the central nervous system (brain and spinal cord), the recommended initial treatment is amphotericin B in combination with flucytosine. After that, fluconazole is recommended for an extended time to clear the infection.
Management and prevention
All patients with cryptococcosis, apart from a few immunocompetent individuals with infection of the lungs, require treatment.
The choice of treatment depends on both the anatomic sites of involvement and the immunological status of the host.
Primary prophylaxis with itraconazole or fluconazole may be effective in HIV-positive patients with a CD4 count of <100 cells/microliter. However, routine antifungal prophylaxis is not recommended because of the infrequency of cryptococcal disease, potential drug interactions, the high cost, the lack of survival benefits associated with prophylaxis, and the potential for development of drug resistance.
However, fluconazole was found to be safe and effective as primary prophylaxis, both before and during early antiretroviral treatment.
Secondary prophylaxis of cryptococcosis involves chronic maintenance therapy with fluconazole as first choice to prevent recurrence of the infection and it may be discontinued in patients who respond to antiretroviral treatment (ART).
It signifies that there is an urgent public health and humanitarian need to conduct trials, and to determine whether antifungal prophylaxis has a role in preventing cryptococcosis and improving survival among HIV-infected persons in developing countries with a high burden of the disease.
References
Srikanta, D., Santiago-Tirado, F. H., & Doering, T. L. (2014). Cryptococcus neoformans: historical curiosity to modern pathogen. Yeast (Chichester, England), 31(2), 47-60.
Gaona-Flores V. A. (2013). Central nervous system and Cryptococcus neoformans. North American journal of medical sciences, 5(8), 492-3.
Ellis, D. H., & Pfeiffer, T. J. (1990). Natural habitat of Cryptococcus neoformans var. gattii. Journal of clinical microbiology, 28(7), 1642-4.
McClelland EE, Hobbs LM, Rivera J, Casadevall A, Potts WK, Smith JM, et al. (2013) The Role of Host Gender in the Pathogenesis of Cryptococcus neoformans PLoS ONE 8(5): e63632. https://doi.org/10.1371/journal.pone.0063632
Alspaugh J. A. (2014). Virulence mechanisms and Cryptococcus neoformans pathogenesis. Fungal genetics and biology : FG & B, 78, 55-8.
Richardson M.D and Warnock D.W. (2003). Fungal Infection- Diagnosis and Management. Third edition. Blackwell Publishing Ltd. Page 240-254.